How Much Protein Do You Need In Nutritional Ketosis?





And why for some people, this is a delicate balance
Protein is a fascinating macronutrient. Of the three dietary macronutrients, protein must provide at least 9 essential components (amino acids), whereas dietary fats provide just 2, and carbohydrates none. To the uninitiated, it is tempting to think of proteins in the body as relatively stable (e.g., the structure of muscles, heart, liver, kidneys, brain) compared to the body’s use of ‘fuel’ (carbohydrate and fat). But in reality the body’s protein metabolism is incredibly dynamic, and limitations in either dietary protein or energy intakes from carbohydrate or fat can tip the balance between gain or loss of important tissues or functions.
When embarking on a well-formulated ketogenic diet and going through the process of keto-adaptation, there are necessary changes in how the body uses its incoming macronutrients to maintain (if not improve) health and function. To achieve this requires enough protein but not too much—balance is important. And as you might expect, this balance is achieved at different ‘recommended daily intake’ levels than our official government recommendations. But as you read this post, you will see that your need for dietary protein during a well-formulated ketogenic diet is not much different from what the average person in the developed world currently eats—i.e., moderate protein rather than high protein (Fulgoni 2008). What follows is our best attempt at a brief explanation of dietary protein requirements during nutritional ketosis.
The dynamics of protein turnover, and why this is important
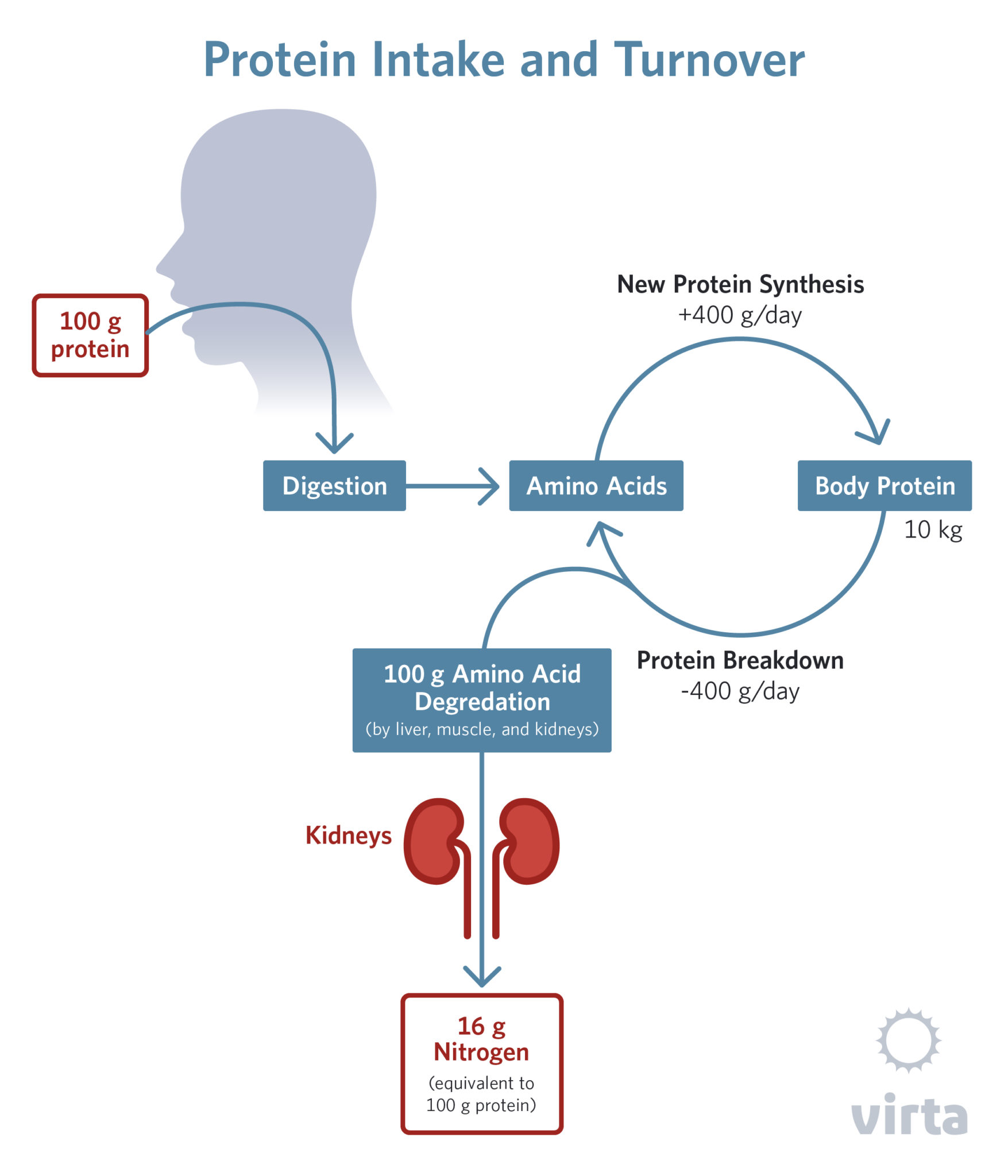
Besides being a vital component of the body’s structure (e.g., muscle, tendon, ligament, bone, skin, hair), it is the stuff from which functional molecules like enzymes, antibodies, membrane receptors and transporters, and oxygen-carrying hemoglobin are made. Every step in your metabolism is accomplished with the help of proteins, which number in the thousands within any one cell. And while some of these last for months once they are made, others last for mere minutes before they are broken down and replaced. In other words, proteins in the body are in a constant dynamic state of being broken down and replaced.Proteins are chemical chains made from 20 different molecules called amino acids, with these chains of amino acids varying in length from less than 10 to many hundreds. On average, the shorter the chain of amino acids, the more rapidly that protein is broken down and replaced. This is called ‘protein turnover’ and it is going on in every cell, tissue, and organ in the body every day. So in order to maintain your health and function, the body needs to be constantly making new proteins. This requires a consistent supply of amino acids and lots of energy, because making new proteins (aka protein synthesis) is a high-energy process.The amino acids that the body uses for protein synthesis come from two sources. The most obvious is the dietary protein that we eat each day, but this is normally the lesser contributor of amino acids for protein synthesis. The major source is actually recycled amino acids from the breakdown of existing body protein. In a typical day when dietary protein and energy intakes are adequate to maintain lean body mass* (i.e., one is neither gaining nor losing lean tissue), more than two-thirds of the amino acids entering the bloodstream come from breakdown of existing body protein, while less than one-third come from digestion and absorption of dietary protein.
*Lean body mass. Body composition is commonly divided into 2 compartments—fat mass and lean body mass. While real life is not quite this simple (e.g., the fat cells in our adipose tissue actually contain about 15% ‘lean tissue’ and 85% stored triglyceride), most of the body’s physiological functions such as circulation, breathing, movement, energy metabolism, conscious and sub-conscious brain activity, digestion, absorption, excretion, and reproduction are performed by our lean (aka non-adipose) tissue. So that’s what most of the body’s protein is used for, right?
Wrong. All of these active things the body does make use about half of its protein, and most of that is inside of our cells. The other half of our protein is structural and is outside of our cells (e.g, tendons, ligaments, bone, skin, hair). But even these proteins are turning over on a regular basis. For example, you replace all of your hair every 2 years, and the outer layer of your skin gets replaced every 3 weeks.
All of these structures and functions are dependent upon having adequate amino acids so that they can rebuild themselves on an ongoing basis, and anything that impairs this rebuilding process over just a few weeks or a few months results in measurable losses of a broad range of functions.
Depending on multiple hormonal and environmental factors, a healthy adult will break down and restore between 300 and 600 grams of protein daily. To put this in perspective, if this were all muscle (which contains about 25% protein and 75% water), that would be the equivalent of replacing between 2.5 and 5 pounds of muscle per day. Actually, much of the body’s protein turnover occurs in tissues other than muscle, but this calculation helps put the magnitude of this process in perspective. And in particular, it should be clear that any factor that gets in the way of protein synthesis (i.e., the ‘rebuilding’ side of this balance equation) can lead to rapid and significant lean tissue loss.
Factors affecting the balance between protein synthesis and breakdown
As shown in the diagram above, some of the amino acids we eat and some that come from protein breakdown are taken up by the liver, kidneys, and muscle where they are metabolized for energy and for purposes other than protein synthesis. In the process, they release the nitrogen molecules that characterize amino acids, and these are mostly excreted as waste nitrogen in the urine. In addition, some protein and protein breakdown products are lost each day from the skin and in feces, but this typically represents about 10% of daily protein losses.
In our dreams, most of us would like to be able to rapidly gain lots of muscle and lose lots of body fat. But in reality, if each morning we wake up with about the same amount of muscle as we had yesterday, we have been able keep protein synthesis and breakdown about in balance, and that’s a good result. When it comes to changes in our protein metabolism, good things happen slowly.
The most rapid changes in protein balance occur with infection, injury, stress, and starvation/fasting. Severe infection and trauma can result in 2–3 pounds of lean tissue loss per day, while up to a pound per day can be lost in the first week of the body’s adaptation to fasting.
On the positive of the protein balance equation, the most rapid gains in lean tissue are seen during recovery from prolonged wasting after illness or starvation, when up to a quarter pound of lean tissue can be added daily. But this rate of gain typically occurs in the context of a high energy (high calorie) diet, usually accompanied by gains in body fat as well. Sustained lean tissue gains are also seen during adolescent growth spurts and in pregnancy. But in the latter case, if the pregnant mother produces a baby containing 3 pounds of lean tissue and adds 5 pounds of lean tissue to her own body over 9 months, that translates to 128 ounces of lean tissue over 180 days, or less than one ounce per day. Additional factors influencing protein balance are listed in the table below, but alone or in combination they rarely result in average lean tissue gains of more than a quarter pound per day.
Factors known to stimulate or facilitate lean tissue gain:
- Exercise (particularly resistance exercise)
- Adequate dietary protein including adequate essential amino acids (usually only a concern with vegan diets)
- Adequate dietary energy (but not necessarily carbohydrate) (Koopman 2007)
- Increased serum insulin (in the presence of adequate amino acids) (Roy 1997, Borsheim 2004)
- Branched chain amino acids
- Adequate intra-cellular minerals (e.g., potassium, magnesium, phosphorus) (Dudrick 1972, WHO, 2005)
- Creatine supplements
- Illegal use of anabolic steroids and growth hormone
In summary, most positive changes in lean body mass occur slowly, whereas losses can occur rapidly with injury, illness, or inadequate dietary protein (including starvation/fasting). In addition, proteins can only be produced when a number of factors are working together, including amino acid availability, associated minerals specific to that tissue, plus appropriate stimulus from hormonal and metabolic signals.
Nutritional ketosis and protein balance
We have known for many decades that lean body mass and physical well-being can be maintained with a ketogenic diet containing a moderate amount of protein. The 1928 Stefansson Bellevue Experiment demonstrated that 2 adult men could eat about 15% of their dietary energy as protein and maintain their weight and function for a year (McClellan 1930). In the modern era, we have done multiple shorter studies with more rigorous body composition analysis yielding similar results (Phinney 1983; Volek 2004). However when making the transition from a high carbohydrate diet to a high fat ketogenic diet, there is a 1–2 week modest lag in protein synthesis as the body switches its primary fuel sources (part of keto-adaptation).
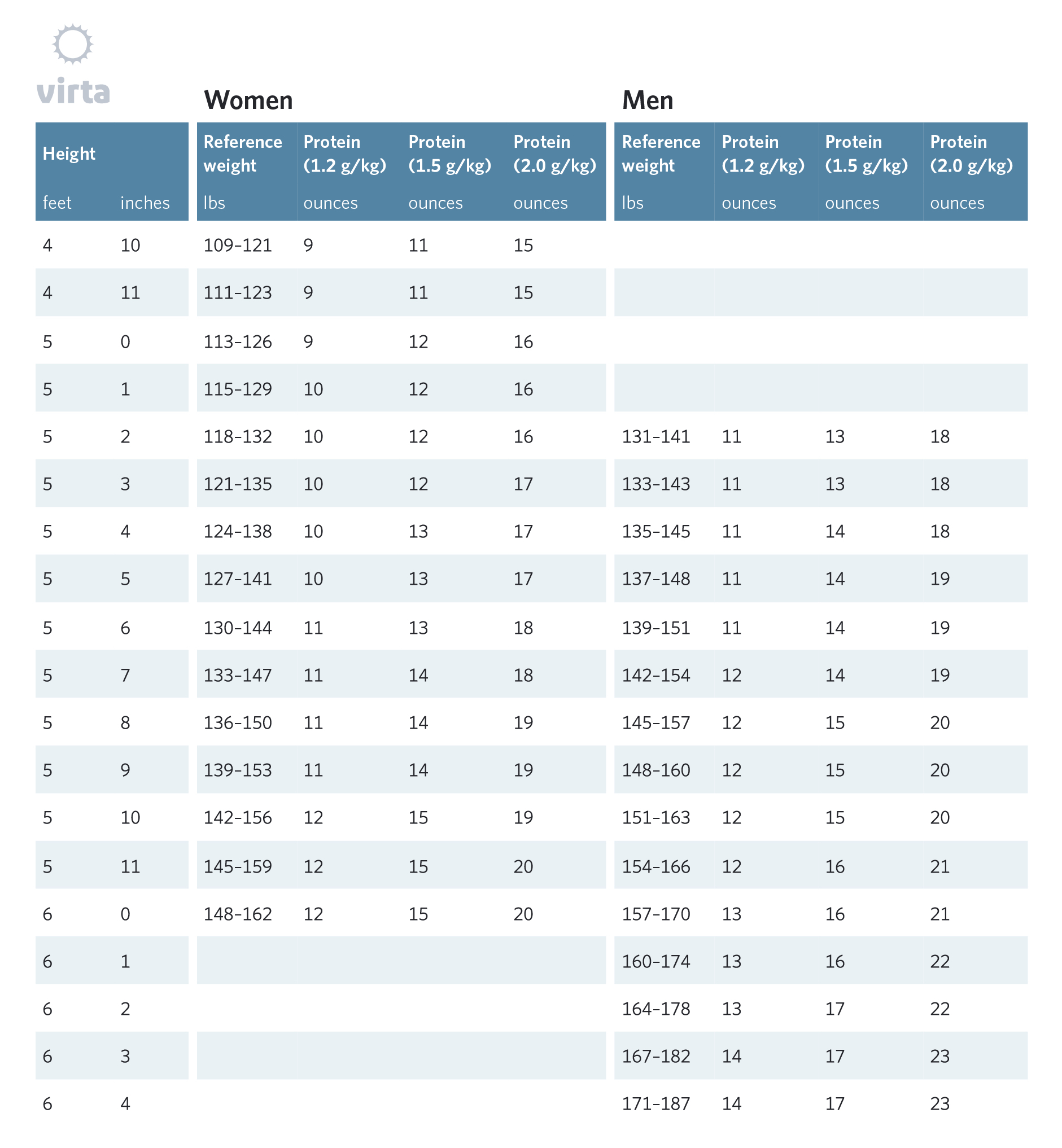
While a precise analysis of dose-response to varying protein intakes during nutritional ketosis has not been done in humans, we have performed a number of studies indicating that most healthy humans maintain lean body mass and function during a ketogenic diet providing between 1.5 and 1.75 grams of protein per kg of ‘reference body weight’* (Phinney 1983, Davis 1990). Furthermore, there are no convincing human studies showing any benefit from dietary protein above 2.0 g/kg reference weight for adults following a ketogenic diet; and any potential benefit from a higher protein intake must be weighed against the reduction in blood ketone levels caused by excess dietary protein (more on this later in this piece).
*Reference body weight is an arbitrary value for men and women based upon the medium frame values from the 1959 Metropolitan Life Insurance ‘Ideal Body Weight’ tables. (Met Life, 1959) Using these values allows for protein intakes to be based roughly on normal lean body mass rather than total body weight. Note: ‘reference weight’ is an arbitrary value used to estimate daily protein needs—it is not a weight
In studies that measure urinary nitrogen excretion, both ketogenic diets and total starvation result in the greatest net protein breakdown in the first week of keto-adaptation. In the case of total starvation, these daily losses range from the equivalent to one half pound to one pound of lean body mass in women and men in the first week (Forbes 1979, Goschke 1975), and then taper towards a quarter pound loss after one month. In contrast, with a well formulated ketogenic diet, these losses average less than one fourth pound per day in the first week and rise to zero loss or even modest tissue gain after 2 weeks of adaptation (Phinney 1983, Davis 1990).
Once through the first few weeks of keto-adaptation, there does not appear to be any reason to change one’s dietary protein intake either with further time of adaptation or cumulative weight loss. The exception would be if blood ketones remain low (i.e., below 0.5 mM) despite tight carbohydrate restriction, in which case reducing protein from the 2.0 to 1.5 g/kg or even to 1.2 g/kg reference weight range might be reasonable.
In our experience, people on a ketogenic diet who think they are eating protein in moderation are often well above 2 g/kg due to fear of eating fat to satiety.
But in no case should dietary protein intake be reduced below 1.2 g/kg in the context of a well-formulated ketogenic diet. This range; 1.2 g/kg at the low end and 2.0 g/kg at the upper end, with a 1.5 g/kg mid-range moderate intake target, can be translated into daily consumption of protein-rich foods in ounces in the table below. Each ounce of protein-containing food contains about 7 grams of protein.
Why are our recommended protein intakes above the RDA of 0.8 g/kg-day?
The Recommended Dietary Allowance (RDA) for protein is defined by an expert committee as the average daily level of intake sufficient to meet the nutrient requirements of nearly all healthy people (NIH). This value for healthy adults who are maintaining at a stable weight is 0.8 grams of protein per kg daily. But it has been noted that this does not take into account illness, calorie restriction, stress, aging, or the minority who need more protein (Wolfe 2017), indicating the need for protein similar to our recommendations. This new perspective in combination with our research indicates that a somewhat higher range covers pretty much all of these added needs when people are following a well-formulated ketogenic diet. In addition, this range is well within the routine intakes of people in the developed world, and thus does not represent a high protein intake in any sense of the word.
Why we don’t use ‘macros’ or ‘percentages’ to guide your protein intake
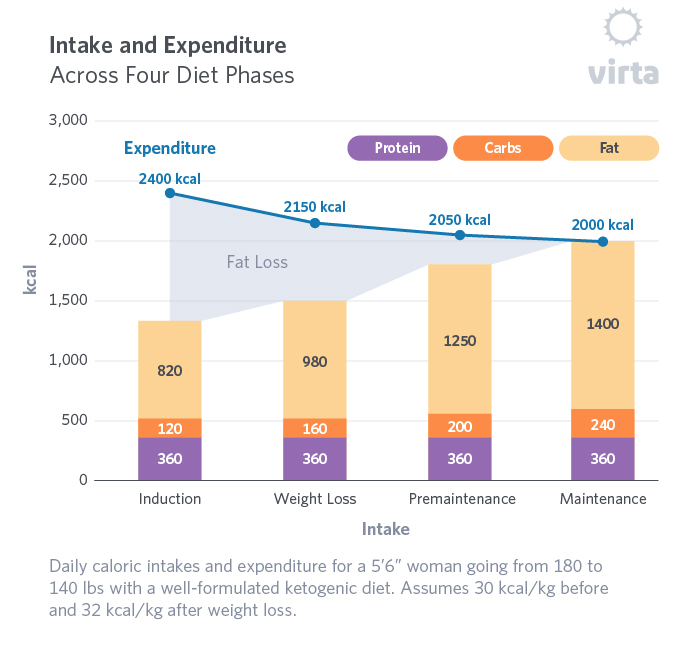
It should be clear from the above explanation that an individual’s protein intake during a well-formulated ketogenic diet is pretty much independent of daily energy intake. For example, an otherwise healthy person beginning a ketogenic diet eaten to satiety usually starts out under-eating calories relative to daily energy needs, and thus loses weight. For example, let’s say that a 5’6” woman with a reference weight of 60 kg starts out at 82 kg (180 lbs) and eats 1300 kcal per day (about a 1000 kcal/day deficit). Her recommended daily protein intake would be 1.5 X 60 = 90 g/day, totaling 360 kcal. Expressed as a ‘macro’ of what’s on her plate, that’s 24% protein. But 6 months later when she weighs 63 kg (140 lbs) and is eating 2000 kcal per day at weight maintenance, that same protein dose (360 kcal out of 2000) represents a protein ‘macro’ of 16%. The point is that in this situation where her weight is changing, her daily protein intake should be constant; whereas her ‘macros’ change as she transitions from weight loss to weight maintenance. This changing proportion of dietary protein to dietary energy as one proceeds through weight loss to weight maintenance is shown in diagram below.
Given the often large changes in body weight and fat mass that usually occur with a well-formulated ketogenic diet, but little if any change in protein requirements as long as one maintains lean body mass and remains in nutritional ketosis, it is better to calculate one’s daily protein need in grams of dietary protein or ‘ounces’ of protein-containing food per day.
Considerations favoring a moderate protein ketogenic diet
A moderate protein intake as part of a well-formulated ketogenic diet allows circulating ketones to reach levels of at least 0.5 mM. Too little or too much protein can negatively impact the many benefits of being in a state of nutritional ketosis. How to determine your protein needs can be a bit of an art and may take some time and expert coaching to get it right.
Too little protein in the diet may increase circulating ketones above 4.0 mM, but at the expense of nitrogen losses which can compromise lean tissue preservation and function. While still well-within the safe ketone range, if you are consistently achieving values above 3.0 mM that cannot be explained by something like exercise, consider modestly increasing your protein intake. In addition to not meeting the body’s needs, a low dietary protein intake can be far less enjoyable than one that is adequate in protein. Two of the many benefits of a well-formulated ketogenic diet are the satiety and satisfaction it provides.
On the other hand, too much dietary protein can drive down ketones for several reasons. Protein has a moderate insulin stimulating effect; and though less than the impact of a similar amount of carbohydrate consumption, high protein intakes can drive down ketone production in the liver (Marliss 1978). In fact, specific amino acids like alanine are potently anti-ketogenic. Additionally, when consumed to excess, protein can upset gastro-intestinal function and place a stress on the kidneys to remove the additional nitrogen.
Mineral considerations
Among the many factors that affect the body’s ability to build and maintain its lean body mass, maintaining an adequate balance of essential minerals is very important. In particular, there are complex inter-relationships among the mechanisms for handling sodium, potassium, and magnesium that can influence the body’s ability to maintain protein-containing tissue and function. (Dudrick 1972, WHO 2005). Without enough of the potassium and magnesium that are concentrated inside our cells, these tissues can’t be built up or even properly maintained. And because inadequate sodium intake causes increased potassium wasting by the kidneys, even salt intake can influence the efficiency with which dietary protein can be used.
In this context, it is also important to understand that our choice of dietary protein and how it is prepared can also influence our essential mineral status. Consuming one’s protein from minimally processed foods, whether from animal or plant sources, generally results in increased intakes of essential minerals. Thus 4 ounces of real chicken, fish, or meat typically contains more than twice the potassium and magnesium found in processed luncheon meats containing the same amount of protein. Boiled meat is leached of its essential minerals unless the broth is consumed, and protein powders such as whey and gelatin tend to be devoid of these important minerals. Ditto that for eggs compared to egg whites. Egg whites contain ‘high biologic value’ protein, but they are devoid of the essential minerals that are concentrated in the yolk. No need to pay more for those egg white omelets!
Conclusions
Achieving and maintaining a protein intake appropriate for a well-formulated ketogenic diet takes practice, and often considerable expert coaching. Individual needs and tolerances may vary, but in almost all cases they are found within the range of 1.2 to 2.0 grams per kg reference body weight. While this range is somewhat higher than the standard recommendations for minimum or average daily requirements, it includes enough of a buffer to allow for recovery after stress, exercise, and the occasional illness. This protein intake level is also consistent with usual protein intakes in developed countries, and matches the protein consumption of aboriginal cultures that consumed a hunter/herder diet for thousands of years. Thus there is no reason to be concerned about long-term consumption of protein in the context of a well-formulated ketogenic diet in someone with normal kidney function.
The information we provide at virtahealth.com and blog.virtahealth.com is not medical advice, nor is it intended to replace a consultation with a medical professional. Please inform your physician of any changes you make to your diet or lifestyle and discuss these changes with them. If you have questions or concerns about any medical conditions you may have, please contact your physician.
This blog is intended for informational purposes only and is not meant to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or any advice relating to your health. View full disclaimer
Are you living with type 2 diabetes, prediabetes, or unwanted weight?

- Borsheim, E., et al., Effect of carbohydrate intake on net muscle protein synthesis during recovery from resistance exercise. J Appl Physiol, 2004. 96(2): p. 674-8.
- Davis PG, Phinney SD. Differential effects of two very low calorie diets on aerobic and anaerobic performance. Int J Obes. 1990 Sep;14(9):779-87.
- Dudrick SJ, Macfadyen, BV Jr, Van Buren CT, Ruberg RL, Maynard AT. Parenteral hyperalimentation. Metabolic problems and solutions. Ann Surg. 1972: 176:259–264.
- Forbes GB, Drenick EJ. Loss of Body Nitrogen on Fasting. Am J Clin Nutr. (1979) 32:1570-1574.
- FAO Joint, World Health Organization Report. Vitamin and mineral requirements in human nutrition. WHO, Geneva Switz. 2005; pp 217-218.
- Fulgoni VL 3rd. Current protein intake in America: analysis of the National Health and Nutrition Examination Survey, 2003-2004. Am J Clin Nutr. 2008
- Goschke H, Stahl M, Tholen H. Nitrogen loss in normal and obese subjects during total fast. Klinische Wochenschrif. 1975;53:605-10.
- Koopman, R., et al., Coingestion of carbohydrate with protein does not further augment postexercise muscle protein synthesis. Am J Physiol Endocrinol Metab, 2007. 293(3): p. E833-42.
- McClellan WS, DuBois EF. Clinical calorimetry: xlv. Prolonged meat diets with a study of kidney function and ketosis. J. Biol. Chem. 1930, 87:651-668.
- Marliss EB, Murray FT, Nakhooda AF. The Metabolic Response to Hypocaloric Protein Diets in Obese Man. J Clin Invest. 1978; 62:468-479. doi:10.1172/JCI109148.
- Metropolitan Life Insurance Company. New weight standards for men and women. Stat Bull Metropol Life Insur Co 1959;40:1–4.
- Phinney SD, et al. The human metabolic response to chronic ketosis without caloric restriction: physical and biochemical adaptation. Metabolism. 1983; 32:757-768.
- Roy, B.D., et al., Effect of glucose supplement timing on protein metabolism after resistance training. J Appl Physiol, 1997. 82(6): p. 1882-8.
- Volek J, Sharman M, Gómez A, Judelson D, Rubin M, Watson G, Sokmen B, Silvestre R, French D, Kraemer W. Comparison of energy-restricted very low-carbohydrate and low-fat diets on weight loss and body composition in overweight men and women. Nutr Metab. 2004; 1:13.
- Volek, JS, Quann, EE, Forsythe CE. Low-Carbohydrate Diets Promote a More Favorable Body Composition Than Low-Fat Diets. Strength & Conditioning Journal. 2010; 32:42-47
- https://ods.od.nih.gov/Health_Information/Dietary_Reference_Intakes.aspx