


Two Year Clinical Trial Outcomes Provide Evidence for Long-Term Benefits of Virta for Type 2 Diabetes




Over fifty percent of adult Americans now have diabetes or pre-diabetes and there are no signs of this epidemic slowing¹. Diabetes has long-been considered a chronic and progressive disease. Treatment of diabetes usually involves recommendations for lifestyle changes, and when lifestyle interventions are insufficient, medications are prescribed to manage the disease and slow progression². Unfortunately, many diabetes medications are costly and some come with undesirable risks and side effects, such as weight gain and increased risk of severe hypoglycemia³,⁴. And despite these treatment efforts, the remission rate under this usual care model is extremely low (0.5-2%)⁵. However, with the right treatment, reversal of hyperglycemia and insulin resistance is possible⁶!
Virta takes a novel approach to diabetes care. We employ a technology-enabled continuous remote care model with individualized guidance for achieving nutritional ketosis. Each patient has a remote care team—a health coach and a medical provider—that continuously customizes their care. Patients also receive behavioral support and encouragement from their coaches and an online community of their peers. We hypothesized that this comprehensive care model would improve health for patients with type 2 diabetes, allowing them to actually reverse hyperglycemia and insulin resistance while removing medications.
To assess the safety, efficacy, and sustainability of the Virta program, we put our treatment to the test in a clinical trial. We enrolled 262 adult volunteers with type 2 diabetes who chose to receive Virta. For comparison, we also enrolled 87 adult volunteers who chose to receive Usual Care for type 2 diabetes, including appointments with their physician and consultations with registered dietitians regarding nutrition and lifestyle changes.
At 1 year, participants who received Virta saw clinically-significant benefits in their health outcomes, such as decreased HbA1c and weight, all while discontinuing 63% of diabetes-specific medications⁷. And while we are very excited about the results after 1 year, we understand that this lifestyle change requires a long-term commitment from our patients. Therefore, we decided to extend our 2-year clinical trial out to 5 years. We are closely following the clinical trial participants to learn more about our care model.
Here we take a look at the 2-year health outcomes of participants in the clinical trial, which were published in Frontiers in Endocrinology, a peer-reviewed journal. At 2 years, 74% of the original 349 trial participants remained enrolled in the trial. We are excited to share that trial participants receiving Virta showed ongoing clinically-significant health improvements at 2 years.
Reversal of diabetic hyperglycemia without use of diabetes-specific medications
The terms Reversal and Remission have both been used to describe regression of hyperglycemia and insulin resistance, but they are defined slightly differently:
- Reversal = Sub-diabetes level glycemia (HbA1c <6.5%) that is achieved without diabetes medications or only with metformin.
- Remission = Similar to reversal, but requires that no diabetes medication (including metformin) be used and that it is maintained for at least 1 year.
Here at Virta, we focus on Reversal. The reason for this is that we believe that it is not in every individual patient’s best interest to arbitrarily stop metformin. Patients who have a history of diabetes remain at increased risk of developing diabetes again, even after HbA1c normalizes, and metformin has been shown to decrease this risk⁸. Therefore, we discontinue metformin only due to side effects or patient request.
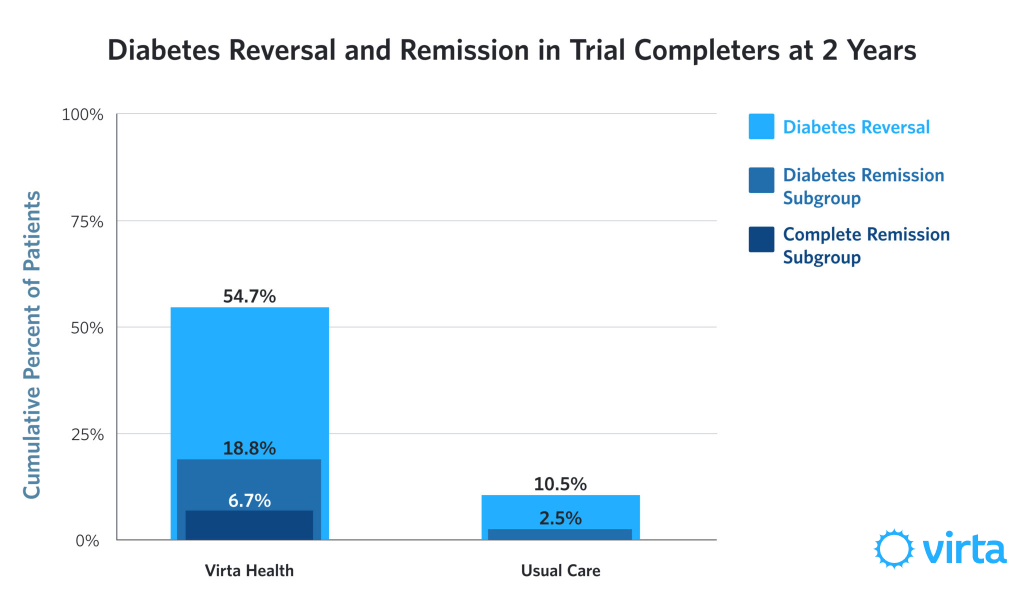
We are thrilled that 55% of Virta participants still enrolled at 2 years achieved Reversal!
Clinically, it might also be important to consider the percentage of patients who achieve Reversal among the total number of patients enrolled at the start of the trial. Those who discontinued participating in the trial or did not complete tests at two years are assumed to have not met Reversal criteria. Using this rigorously conservative approach, 38% of the 262 participants who began the trial met criteria for Reversal at 2 years.
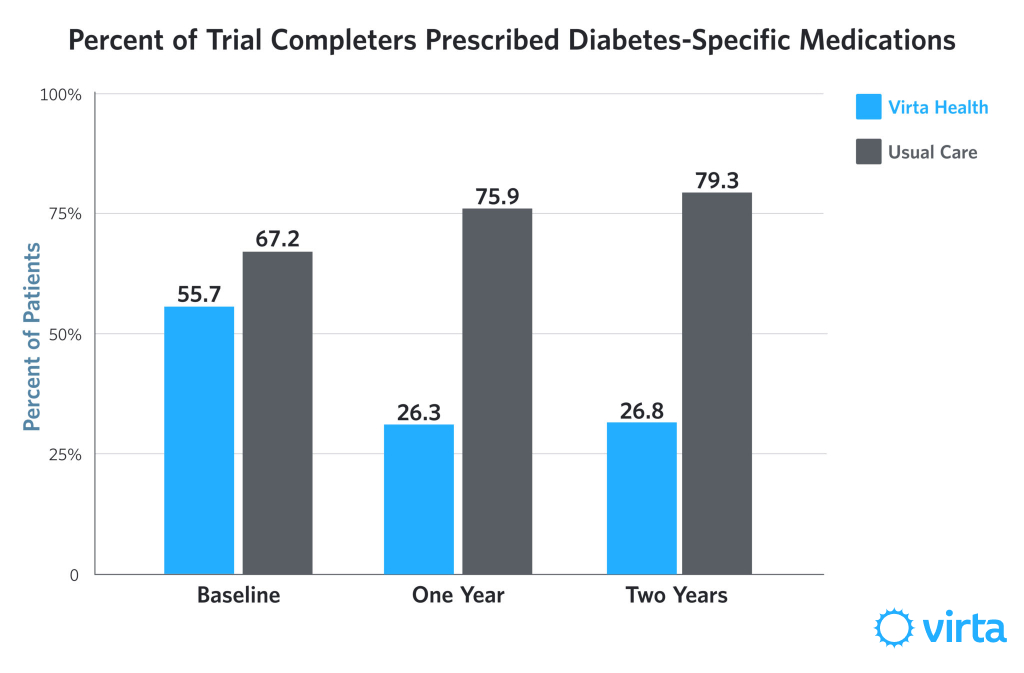
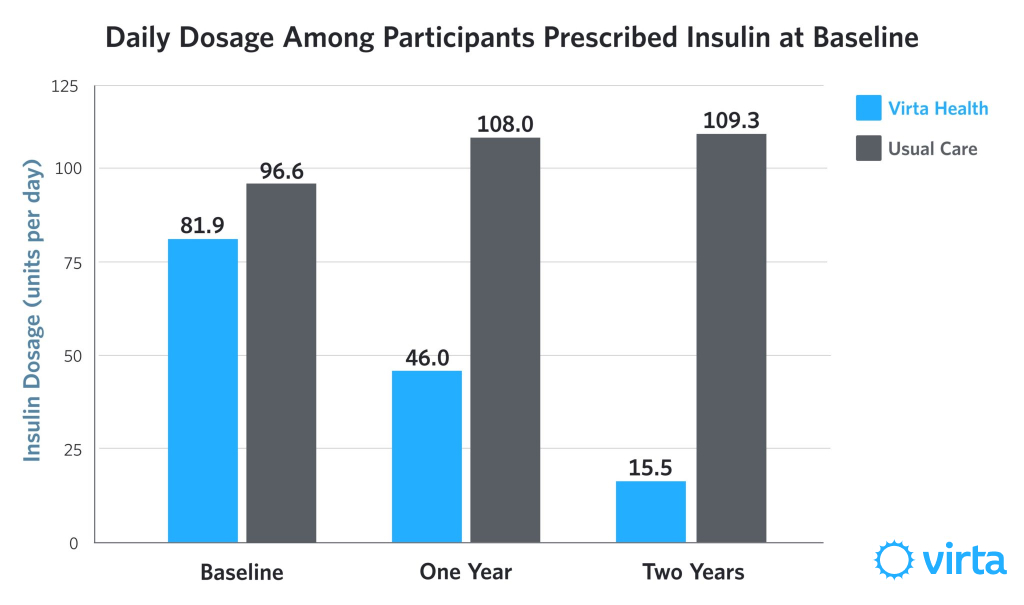
At 2 years, participants who received Virta maintained reductions in diabetes-specific medication use. In fact, average daily insulin dosage further declined at 2 years.
Trial participants on Virta also continued to show clinically-significant improvement in HbA1c from baseline to 2 years.
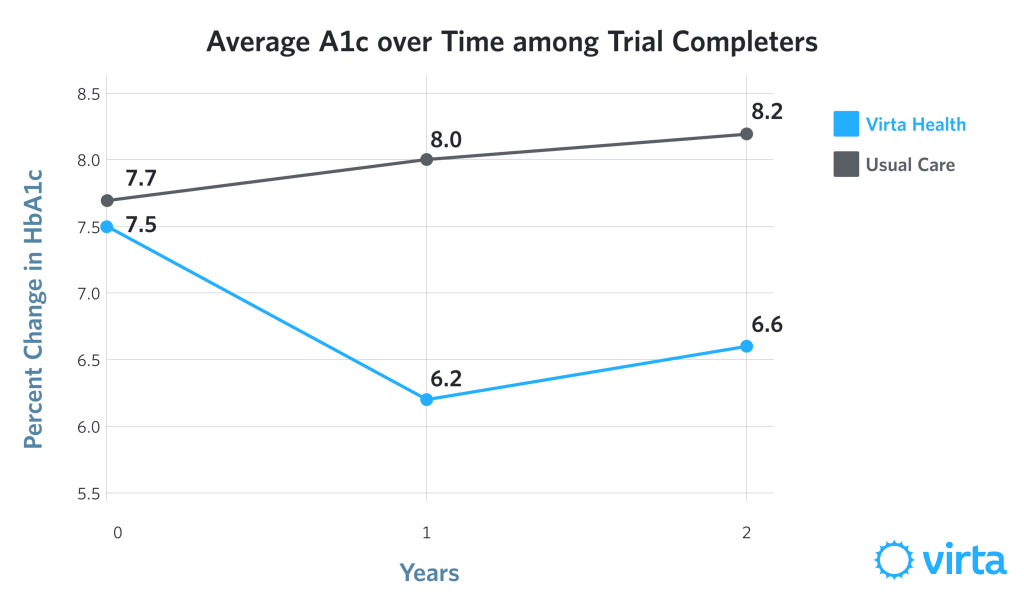
Sustainability
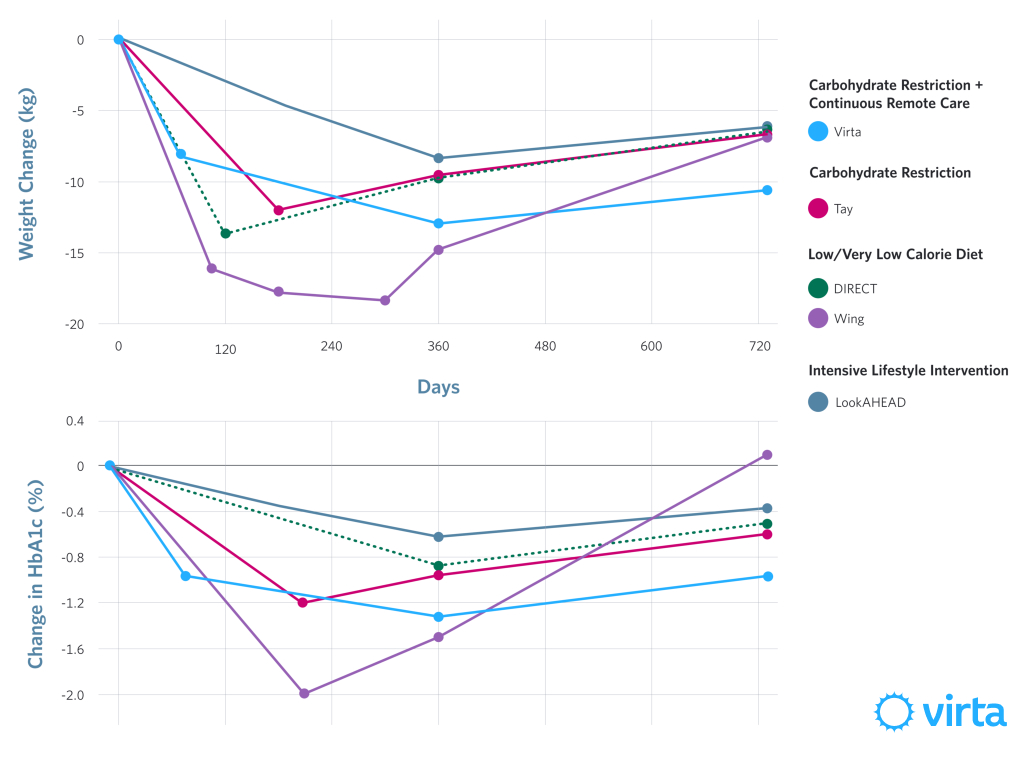
You may have noticed a slight increase in HbA1c between years 1 and 2. We also saw a slight increase in weight (5 pounds on average). This is an issue for any lifestyle change intervention. Many brilliant researchers have spent their entire careers working to improve sustainability. Most lifestyle intervention studies see regression towards baseline values within the first year, and then major, if not total, regression to baseline at 2 years. After 2 years in our study, our participants' average reduction in HbA1c and weight was about two times that of comparable study populations (see below)⁹,¹⁰,¹¹,¹².
In this trial, participants’ average ketone levels (which indicate adherence to a low-carbohydrate diet) remained significantly increased over baseline at 2 years, meaning that overall participants continued to restrict carbohydrates at 2 years. This provides evidence of long-term sustainability of this lifestyle. We can’t be certain about what has led to our study participants maintaining improvements at such a high rate. We believe that it is likely a combination of a satisfying diet that does not require calorie counting combined with the continuous support and monitoring with individualized recommendations for carbohydrate restriction.
Impact beyond type 2 diabetes
Safety is our top priority at Virta. In addition to diabetes, we monitor other aspects of our participants’ health to ensure other health risks are unaffected, or even better, improving! Our goal is to make patients healthier overall.
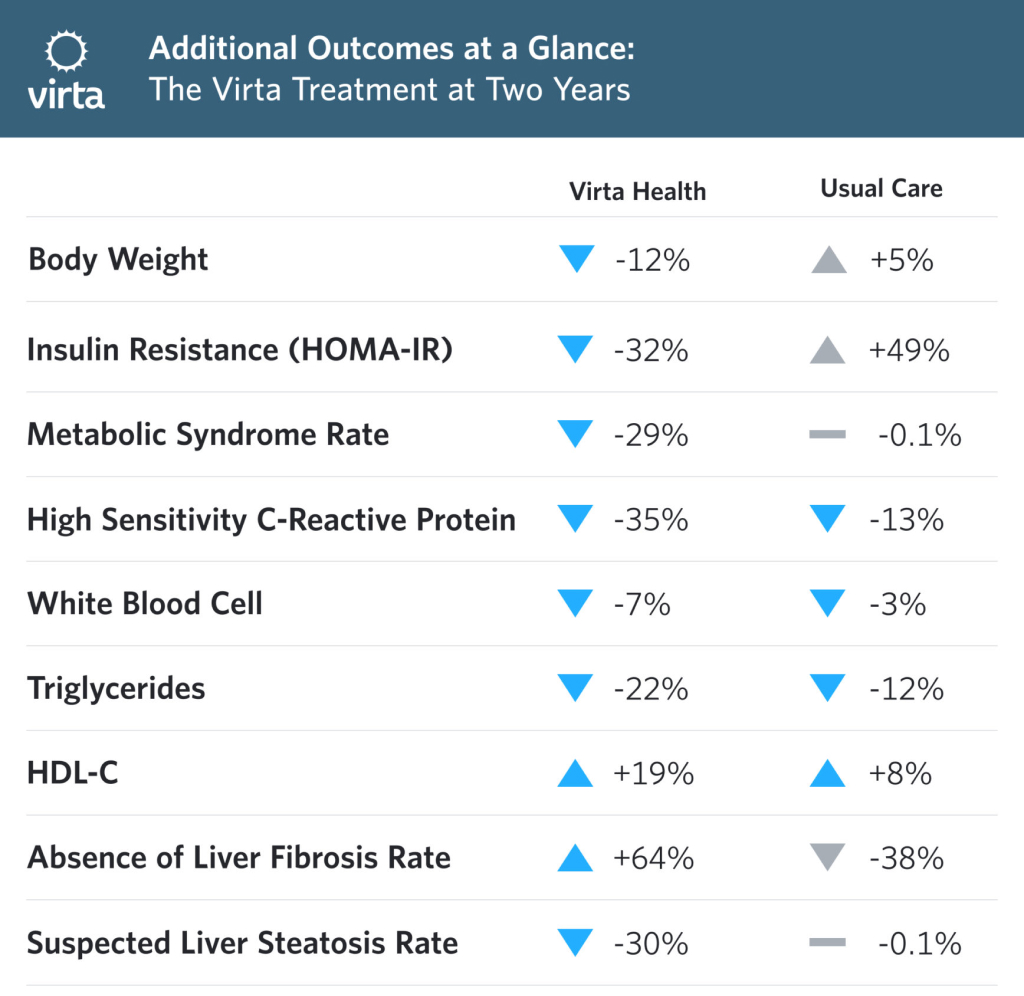
Not only can the Virta program be delivered without negative impact on other aspects of health, it also improves other health conditions that commonly co-occur with diabetes such as inflammation, insulin resistance, dangerous (atherogenic) changes in blood lipids, and fatty liver disease. Among Virta participants still enrolled at 2 years, 75% had lost at least 5% of their body weight and 50% had lost over 10%. This is in contrast to the Usual Care group, who showed no significant improvement in their diabetes status or other health markers.
Take-home points
- Participants receiving Virta had long-term clinically-significant improvement in glycemic outcomes alongside reduced medication usage.
- A high percentage of participants receiving Virta met criteria for remission compared to what we see under usual care and even in other intensive lifestyle interventions¹²,¹³.
- Participants receiving Virta sustained clinically-significant weight loss at 2 years.
- Virta is safe. Participants had improvements in risk factors for other health conditions
This blog is intended for informational purposes only and is not meant to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or any advice relating to your health. View full disclaimer
Are you living with type 2 diabetes, prediabetes, or unwanted weight?

- Menke, A., Casagrande, S., Geiss, L., & Cowie, C. C. (2015). Prevalence of and trends in diabetes among adults in the United States, 1988-2012. JAMA, 314, 1021-1029.
- Bethel, M. A., Patel, R. A., Merrill, P., Lokhnygina, Y., Buse, J. B., Mentz, R. J., ... & Maggioni, A. P. (2018). Cardiovascular outcomes with glucagon-like peptide-1 receptor agonists in patients with type 2 diabetes: A meta-analysis. The Lancet Diabetes & Endocrinology, 6, 105-113.
- Action to Control Cardiovascular Risk in Diabetes Study Group. (2008). Effects of intensive glucose lowering in type 2 diabetes. New England Journal of Medicine, 358, 2545-2559.
- Henry, R. R., Gumbiner, B., Ditzler, T., Wallace, P., Lyon, R., & Glauber, H. S. (1993). Intensive conventional insulin therapy for type II diabetes: Metabolic effects during a 6-mo outpatient trial. Diabetes Care, 16, 21-31.
- Karter, A. J., Nundy, S., Parker, M. M., Moffet, H. H., & Huang, E. S. (2014). Incidence of remission in adults with type 2 diabetes: the diabetes & aging study. Diabetes Care, 37(12), 3188-3195.
- Boden, G., Sargrad, K., Homko, C., Mozzoli, M., & Stein, T. P. (2005). Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes. Annals of Internal Medicine, 142, 403-411.
- Hallberg, S. J., McKenzie, A. L., Williams, P. T., Bhanpuri, N. H., Peters, A. L., Campbell, W. W., ... & Volek, J. S. (2018). Effectiveness and safety of a novel care model for the management of type 2 diabetes at 1 year: An open-label, non-randomized, controlled study. Diabetes Therapy, 9, 583-612.
- Diabetes Prevention Program Research Group. (2019). Long-term effects of metformin on diabetes prevention: identification of subgroups that benefited most in the Diabetes Prevention Program and Diabetes Prevention Program Outcomes Study. Diabetes Care, 42, 601-608.
- Tay, J., Thompson, C. H., Luscombe‐Marsh, N. D., Wycherley, T. P., Noakes, M., Buckley, J. D., ... & Brinkworth, G. D. (2018). Effects of an energy‐restricted low‐carbohydrate, high unsaturated fat/low saturated fat diet versus a high‐carbohydrate, low‐fat diet in type 2 diabetes: A 2‐year randomized clinical trial. Diabetes, Obesity and Metabolism, 20, 858-871.
- Lean, M. E., Leslie, W. S., Barnes, A. C., Brosnahan, N., Thom, G., McCombie, L., ... & Rodrigues, A. M. (2019). Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. The Lancet Diabetes & Endocrinology, 7, 344-355.
- Wing, R. R., Blair, E., Marcus, M., Epstein, L. H., & Harvey, J. (1994). Year-long weight loss treatment for obese patients with type II diabetes: does including an intermittent very-low-calorie diet improve outcome?. The American Journal of Medicine, 97, 354-362.
- Look AHEAD Research Group. (2010). Long term effects of a lifestyle intervention on weight and cardiovascular risk factors in individuals with type 2 diabetes: Four year results of the Look AHEAD trial. Archives of Internal Medicine, 170, 1566.
- Esposito, K., Maiorino, M. I., Petrizzo, M., Bellastella, G., & Giugliano, D. (2014). The effects of a Mediterranean diet on the need for diabetes drugs and remission of newly diagnosed type 2 diabetes: Follow-up of a randomized trial. Diabetes Care, 37, 1824-1830.





