Is There a Role for Short-Term Ketosis in Long-Term Care for Type 2 Diabetes?




Weight loss is the standard first step prescribed for overweight people with type 2 diabetes. However, this is notoriously difficult when blood insulin levels are high due to the disease itself, the use of injected insulin, or to diabetes medications that increase insulin production. These factors are further exacerbated by the typically prescribed low-fat diet containing refined carbohydrates and simple sugars that increase the demand for insulin.
In contrast to this current standard of care, severely restricting dietary carbohydrate has been shown in multiple studies to promptly lower insulin levels and improve blood glucose control, thus facilitating weight loss (1, 2). In its most aggressive form, a combination of severely restricting both carbohydrates and calories has led to the development of semi-starvation very low calorie diets (VLCD), typically providing 800 kcal or less per day. While a VLCD can consist of low-carbohydrate, low-fat whole foods (3); commercial VLCDs are typically formula diets composed of chemically pure nutrients mixed together as a packaged powder that can be reconstituted with water and consumed as a beverage, soup, or pudding. These VLCDs have been commonly used for rapid weight loss, and in some cases in people with T2D, but there is no clear consensus on if and how such a rapid weight loss intervention can be harnessed to serve the long term management or reversal of this chronic disease.
In this post, we will examine the potential role of a VLCD in the management (if not reversal) of T2D as a chronic disease, and compare its efficacy to that of a well-formulated ketogenic diet. In particular, we will ask if there is credible published evidence for a natural or plausible transition from a semi-starvation VLCD to a weight-maintaining pattern of eating that allows a majority of patients to maintain a reduced body weight and better control of their diabetes long-term.
A Brief Metabolic Perspective
Since insulin was discovered almost a century ago, the existence of measurable circulating blood ketones (aka ‘ketonemia’) has been anathema to most healthcare practitioners. The logic behind this was that untreated ketoacidosis is fatal and injected insulin can reverse ketonemia. Given the diagnostic assays of that time, the moderate ketonemia due to nutritional ketosis was not easily differentiated from ketoacidosis, so nutritional ketosis ended up as collateral damage from the discovery of insulin. This stands in stark contrast to the prior century, during which some combination of fasting and a carbohydrate restricted diet was the only effective treatment for diabetes (4).
With the development of a more precise insulin assay and thus the ability to accurately determine circulating insulin levels, we have come to appreciate the underlying role of insulin resistance in type 2 diabetes. Yet somehow, the use of injected insulin and medications that increase the endogenous production and secretion of insulin have remained mainstays in the management of this disease.
We have observed that patients with insulin resistance require larger insulin dosages because circulating insulin levels need to be much higher in order to control blood glucose than the levels typically needed in insulin sensitive individuals. Given insulin’s dominant role in managing the storage (and at reduced levels, mobilization) of body fat, these supra-physiologic insulin levels end up contributing to obesity, ectopic fat storage, and hepatic steatosis. This was definitively demonstrated with the Diabetes Control and Complications Trial/ Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) study that looked at intensive glucose control in patients with type 1 diabetes (5). In this study, the improved glucose control was accompanied in the short-term by substantial weight gain and in the long-term by persistent central obesity, dyslipidemia, and atherosclerosis.
Ground-Breaking Studies from Decades Past
Despite the mainstream focus on injected insulin and insulin secretagogues during the 20th Century, there remained a modicum of interest in the use of carbohydrate restriction, particularly in patients with obesity-associated diabetes. The interest that did exist largely involved research on VLCDs due to the assumption that weight loss, per se, was the primary driver that improved diabetes control. Salient amongst these studies were:
- An inpatient metabolic ward study by Bistrian et al. (3) in which 7 insulin-using patients with T2D were given diets composed of real food (lean meat, fish, poultry) ranging from 200-600 kcal/day. Injected insulin was withdrawn in a mean of 9 days due to improved blood glucose control. Initial weight loss was rapid, and subjects were discharged to out-patient follow up after (1-4) weeks. Five of the 7 subjects maintained substantial weight loss and remained off insulin after 1 year.
- A randomized controlled, 12-month trial by Wing et al. of 93 outpatients with T2D (one quarter using insulin) compared two interventions, one using an intermittent VLCD compared to a group assigned a low-fat 1200 kcal diet of common food for the entire trial duration (6). The intermittent VLCD group consumed a 400-500 kcal VLCD prepared formula for the first 12 weeks, followed by 12 weeks consuming a 1200 kcal common food diet, then returned for another 12 weeks on the 400-500 kcal VLCD formula, and finally finishing the study on the 1200 kcal common food diet. Weight loss was greater for the VLCD group in the first 12 weeks, which then persisted to the end of the initial 12-month study. After 2 years, however, both groups had regained more than half of their initial weight losses. Although HbA1c reductions did not differ between the two groups at 1 year, diabetes medication use was less in the VLCD group at this time point. After 2 years, however, both groups’ HbA1c values had returned to their baseline diabetic levels.
What these prior VLCD studies were able to show is that for obese humans, carbohydrate-restricted diets under 800 kcal/day were very powerful at improving T2D control, but the transition back to a ‘balanced’ diet composed of common food was difficult and in most cases did not result in improved T2D control after 2 years. Table 1 below summarizes the differences in composition and use of a VLCD compared to a well-formulated ketogenic diet.
Table 1.Formula VLCDWell-Formulated KDMacronutrient SourcePurified NutrientsReal foodDaily Energy Intake kcal400-800+Eaten to satietyProtein g/kg ref wt0.6 - 1.01.2 -2.0Carbohydrate g/dFixed ratio, 30-100Individualized 20-60Fat g/dFixed ratio 2-30Eaten to satietyKetogenic?Variable - depends on carbYesDurationUsually 2-5 months maxOpen ended, out to yearsMaintenance strategyTransition to ‘healthy food’Eat WFKD to satietyEffect on REEPrompt decline 10-15%No effect at 12 weeks
Something Old, Something New: VLCDs vs Well Formulated Ketogenic Therapy in the 21st Century
There has been an accelerating rate of research interest in nutritional ketosis in the last 20 years, and it is segregating itself into three general topics: 1) the safety of sustained ketosis, 2) beta-hydroxybutyrate (the predominant ‘ketone’) as a beneficial signaling molecule, and 3) the method and duration of inducing nutritional ketosis. We have previously addressed questions about the feasibility and safety of sustained ketosis and BOHB, but two recent studies have re-kindled some questions. Does using some form of a VLCD to jump start the benefits of ketosis in patients with T2D result in lasting advantages? Or, given the recently published results from our Virta/IUH study, do the data available indicate that starting with a well-formulated ketogenic diet therapeutic approach may be inherently more sustainable? Here in brief are summaries of two reports using a short-term VLCD in patients with type 2 diabetes.
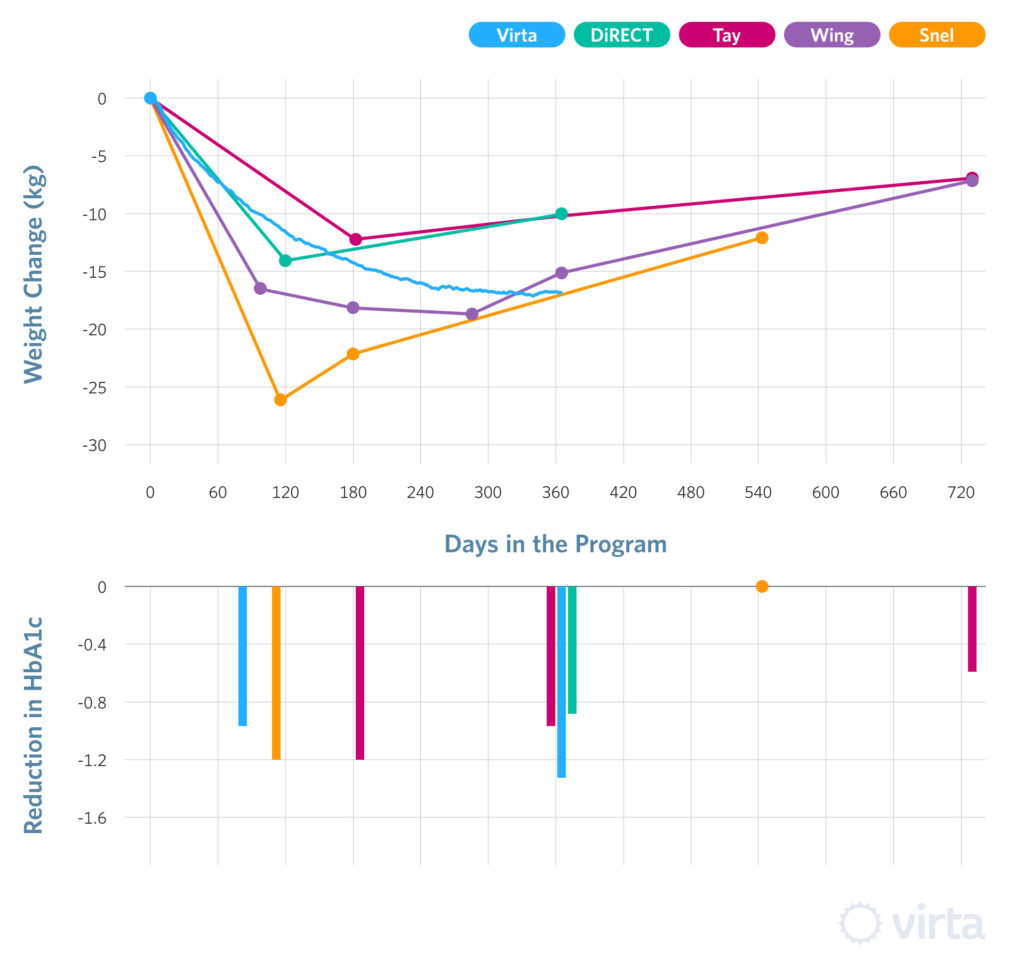
The Leiden VLCD Diabetes Study (7). A Dutch group recruited 27 insulin-using patients with T2D into a single-arm study in which all subjects were administered a 450 kcal/day ketogenic formula VLCD for from 3-4 months. During months 5-6, they were transitioned back to a common-food diet following Dutch healthy eating guidelines. The initial weight loss and HbA1c responses are shown in figure 1, which also shows the subjects’ responses to refeeding after a year – i.e., a total of 18 months into the protocol. Weight losses were dramatic after 4 months on the VLCD, as were reductions in the mean HbA1c values. However, after 12 months of refeeding, both the initial weight loss and improvements in glucose control, as indicated by HbA1c values, had regressed all the way back to baseline.
The Northern UK/Scotland DiRECT Study (8). This large study is described as a cluster-randomized controlled trial evaluating a formula VLCD providing 850 kcal/day administered for 3-5 months to non-insulin-using patients with recent-onset T2D. The control population was a matched group of patients in similar primary care practices who chose to continue usual care for their T2D. While the practices were randomized for the treatments offered (VLCD vs usual care), in both cases the patients knew in advance which treatment they were signing up for. Thus the actual blinding in this study applied only to the statisticians who evaluated the data. In total, 306 patients in 49 practices were recruited. Following 3-5 months on the prepared formula diet (described as providing 55 g/d protein and 125 g/d carbohydrate – thus marginally ketogenic based on the caloric restriction), the patients were then transitioned back to a common-food diet described as:
“Structured food reintroduction of 2–8 weeks (about 50% carbohydrate, 35% total fat, and 15% protein), and an ongoing structured program with monthly visits for long-term weight loss maintenance” (8).
Weight loss and HbA1c values are shown in figure 1. Although hard to ascertain from the published data, it appears that the mean weight loss for the formula VLCD group was 14.5 kg after 3-5 months, but then regressed to 10 kg after 1 year (i.e., after 7-9 months of refeeding). Two-year outcome data from this study have yet to be published.
The IUH/Virta Diabetes Reversal Study (2, 9). This study design was similar to the DiRECT Study, in that intervention and control sites were identified (in our IUH Study consisting of 1 each) and patients at each site recruited independently in parallel. However, as shown in Table 1, the low carbohydrate interventions were quite different. These differences included:
- The IUH/Virta patients were counseled by remote continuous care from day 1 to consume a low carbohydrate, moderate protein diet with fat to satiety – i.e., there was no imposed energy restriction or calorie counting.
- There were just two medical practices involved – one that offered the well-formulated ketogenic therapeutic treatment and one that did not.
- It was clear at the time of recruitment that the doctors and patients were aware of what group they were signing up for.
- There was no attempt to ‘power the study’ for group size based upon expected outcomes because prior data would have indicated that for P<0.01 the primary outcome would be expected to differ with N<20. But to assess less common side effects and secondary outcomes, the recruitment goals were set at 400 for the remote continuous care ketogenic treatment and 100 for the usual care controls.
- The diabetes and pre-diabetes treatment ‘N’ was almost 3 time greater than the DiRECT study VLCD population.
- The IUH/Virta dietary counseling is intended to guide patients to sustain nutritional ketosis for the planned 5-year duration of this study. Patients get access to one-on-one, on-demand health coaching and are supervised by a physician.
- The IUH/Virta subjects (which included patients using insulin) had a mean duration of diabetes diagnosis that was 3 times that of the DiRECT Study.
The results for weight loss and HbA1c values for these three similar studies are shown in Figure 1. Admirably, patient retentions after 12-18 months in all three studies were similarly above 80%. Initial weight losses favored the Leiden VLCD cohort, while the IUH/ Virta and DiRECT groups were similar at around 14-15 kg. After 1 year however, weight regain had begun for both the Leiden and DiRECT groups, whereas the IUH/Virta cohort achieved weight stability between 8 and 12 months. Finally, and perhaps most importantly, The IUH/Virta remote continuous care cohort sustained blood ketone levels significantly greater than their baseline values after 1 year of this intervention (2).
FIGURE 1
Weight loss is a primary metric in most intervention studies involving obese patients with T2D, although we view weight loss as a secondary benefit to the metabolic health effects of the Virta treatment. In this regard, ketogenic diets are too often viewed in the context of “weight loss diets” without taking into consideration all of the health benefits and advantages that accompany ketones and nutritional ketosis. While losing weight is an important outcome, the sustainability of weight loss, glycemic control and the concomitant improvements in metabolic health are more valuable.
So, what have we learned by comparing these recent interventions using VLCDs or a well-formulated ketogenic diet? We know that medically-monitored VLCD diets can be a powerful tool to jump start weight loss and blood glucose control in obese patients with T2D (10). And in fact, many VLCD interventions result in near immediate improvements in glycemic control (6, 10, 11). However, these improvements are rarely maintained at the level that was initially achieved with the VLCD over the ensuing 12-24 months (6, 7, 8, 12). In an effort to refocus the approach of the treatment of T2D towards a reversal of the disease rather than management of the symptoms, an emphasis on sustained glycemic control becomes the most important metric when evaluating the efficacy of an intervention.
The transient nature of metabolic benefits and the trend towards weight regain that promptly follows these VLCD studies points to the time that patients are transitioned off of these artificial diets as a particularly vulnerable period. Perhaps the benefits of ketosis and glycemic control that were achieved following these interventions could set the stage for continued improvement if the patients were transitioned differently. One potential strategy that has yet to be studied would be to follow the formula VLCD with a ketogenic diet composed of whole foods eaten to satiety.
In a previous blog post, we defined a well-formulated ketogenic diet wherein we described that lasting metabolic improvements require a coordinated plan of monitoring and support to enable the patient to reintegrate their lifestyle with real, whole foods and sustainable eating patterns. Without this, the fraction of patients who maintain the initial weight loss and glycemic control benefits is distressingly low (6, 7). In contrast, after one year, our Virta/IUH study remote continuous care cohort has maintained their HbA1c and weight reductions. Therefore, a well-formulated ketogenic diet may produce more sustainable results while allowing the patient to remain in nutritional ketosis thus increasing long-term health benefits via the combined fueling and epigenetic roles of ketones like beta-hydroxybutyrate.
The Side Benefits of Nutritional Ketosis
Starting 5 years ago with a seminal paper by Shimazu et al. in Science (13), we have recently come to appreciate beta-hydroxybutyrate (BOHB) as an ancient fuel and hormone that provides and promotes clean energy metabolism throughout the body. BOHB enables the body’s inborn antioxidant functions through class-1 HDAC down-regulation (a hormone-like activity), while at the same time generating mitochondrial ATP with less than half the secondary reactive oxygen species production compared to glucose (14). BOHB is also a specific inhibitor of the NLRP3 inflammasome assembly which has important implications with respect to diseases caused by chronic inflammation (15).
Some of the profound benefits of nutritional ketosis that were observed in the Virta/IUH intervention subjects were an astounding 39% reduction in serum C-reactive protein after 1 year, and a similarly significant reduction in circulating white blood cell count. Both of these measures of inflammation are positively associated with type 2 diabetes, coronary heart disease, most common cancers, and Alzheimer’s disease; therefore these reductions are likely associated with dramatically reduced chronic disease risks.
Interim Conclusions
Formula very-low calorie diets (VLCDs) have been shown to dramatically reduce body weight and improve glycemic control in individuals with T2D in both inpatient and outpatient studies. However, follow up of outpatient studies using VLCDs in individuals with T2D typically result in weight regain and loss of glucose control as early as 3-6 months after adopting a non-ketogenic weight maintenance diet. When looking at the therapeutic value of BOHB as both a metabolically preferred fuel and as a signaling molecule, it is reasonable to conclude that transiently ketogenic dietary strategies can only be expected to yield transient benefits. In contrast, our 1-year results indicate that a well-formulated ketogenic diet therapy delivered by remote, continuous care yields sustained metabolic benefits, including sustained weight loss and reversal of T2D in the majority of our patients (2).
The information we provide at virtahealth.com and blog.virtahealth.com is not medical advice, nor is it intended to replace a consultation with a medical professional. Please inform your physician of any changes you make to your diet or lifestyle and discuss these changes with them. If you have questions or concerns about any medical conditions you may have, please contact your physician.
This blog is intended for informational purposes only and is not meant to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or any advice relating to your health. View full disclaimer
Are you living with type 2 diabetes, prediabetes, or unwanted weight?

- Boden, G., Sargrad, K., Homko, C., et al. Effect of a Low-Carbohydrate Diet on Appetite, Blood Glucose Levels, and Insulin Resistance in Obese Patients with Type 2 Diabetes. Annals of Internal Medicine. 2005; 142(6):4013-412
- Hallberg, SJ., McKenzie, AL., Williams, PT., et al. Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. Diabetes Ther. 2018; 9:583–612
- Bistrian BR, Blackburn, GL.,Flatt, JP., et al. Nitrogen Metabolism and Insulin Requirements in Obese Diabetic Adults on a Protein-Sparing Modified Fast. Diabetes.1976; 26(6):494-504
- Joslin EP. The treatment of diabetes mellitus. Canadian Med Assoc J. 1916; 6:673-684.
- Purnell,JQ., Hokanson,JE., Cleary,PA., et al. The Effect of Excess Weight Gain with Intensive Diabetes Treatment on Cardiovascular Disease Risk Factors and Atherosclerosis in Type 1 Diabetes: Results from the Diabetes Control and Complications Trial / Epidemiology of Diabetes Interventions and Complications Study (DCCT/EDIC) Study. Circulation. 2013; 127(2)
- Wing, RR., Blair, E., Marcus, M., et al. Year-Long Weight Loss Treatment for Obese Patients with Type II Diabetes: Does Including an Intermittent Very-Low-Calorie Diet Improve Outcome? The American Journal of Medicine. 1994; 97:354-362
- Snel, M. The Effects of a Very Low Calorie Diet and Exercise in Obese Type 2 Diabetes Mellitus Patients. (Unpublished Doctoral Thesis) Leiden University. 2011
- Lean, MEJ., Leslie, WS., Barnes, AC. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomized trial. Lancet. 2018; 391: 541–51
- Bhanpuri , NH., Hallberg, SJ., Williams, PT., et al Cardiovascular disease risk factor responses to a type 2 diabetes care model including nutritional ketosis induced by sustained carbohydrate restriction at 1 year: an open label, non-randomized, controlled study. Cardiovasc Diabetol (2018) 17:56
- Rothberg, AE, McEwen, LN, Kraftson, AT, et al. Very-low-energy diet for type 2 diabetes: An underutilized therapy? J Diabetes Complications. 2014; 28(4):506-510
- Gumbiner, B., Wendel, JA., McDermott, MP. Effects of diet composition and ketosis on glycemia during very-low-energy-diet therapy in obese patients with non-insulin-dependent diabetes mellitus. Am J Clin Nutr. 1996; 63:110-5
- Tay, J., Thompson, CH., Luscombe-Marsh, ND., et al. Effects of an energy-restricted low-carbohydrate, high unsaturated fat/low saturated fat diet versus a high-carbohydrate, low-fat diet in type 2 diabetes: A 2-year randomized clinical trial. Diabetes Obes Metab. 2018; 20(4):858-871
- Shimazu, T., Hirschey, MD., Newman, J., et al. Suppression of Oxidative Stress by Beta-Hydroxybutyrate, an Endogenous Histone Deacetylase Inhibitor. Science. 2013; 11; 396(6116):211-214
- Newman J, Verdin E. Beta-hydroxybutyrate: More than a Metabolite. Diabetes Res Clin Pract. 2014. 106(2):173-181
- Youm, YH., Nguyen, KY., Grant, RW., et al. Ketone body Beta-hydroxybutyrate blocks the NLRP3 inflammasome-mediated inflammatory disease. Nat Med. 2014; 21(3):263-269